Miss Dickson is a 23 year old woman who was admitted to hospital for the purpose of newly diagnosed acute monocytic Leukemia requiring urgent treatment.
Candace was well until June 2013 when she developed a viral infection. This did not improve over time and she presented to the emergency department in St. Catharines where she was admitted with elevated liver function tests as well as leukopenia and thrombocytopenia. At the time, her total WBC count was 1.5 with a neutrophil count of 0.1 and platelets 82. A multitude of investigations were done which were essentially normal and her white count and platelets recovered. She was well until mid December when she began to have lower quadrant abdominal pain, urinary urgency and one episode of night sweats. She was treated with Septra for a UTI. Her symptoms did not improve and she presented to the ED in early January where a pelvic ultrasound was done. This was thought to be on the basis of Pelvic inflammatory disease and she was given ceftriaxone, doxycycline and metronidazole. She was discharged home and developed profuse diarrhea, vomiting, malaise and bone pain. Around this time, she also developed a mass in her left breast. She continued to feel unwell and re-presented to the ED on January 13. At that time, her WBC count was quite elevated at 36 with neutrophil count of 9.9, lymphocyte count of 17.9 and monocyte count of 6.7. Platelets were 35 and hemoglobin was 113. Her LDH was above 2000. Her creatinine was 92. On the second day it was 115. By the third day it had risen to 147. Non contrast CT scan was done which showed extensive retroperitoneal adenopathy with bulky nodes in the iliac chains, moderate right sided pleural effusion, thrombus in the portal vein as well as a hypoechoic lesion behind the bladder measuring 8.9 x 8.3cm and mild bacterial hydronephreosis. At this time, she became oliguric. She was given a dose of rasburicase and seen by Nephrology, and received urgent dialysis. A bone marrow aspirate and biopsy was also completed which demonstrated 80% blast cells consistent with a monocytic variant of Leukemia. She was transferred to the Juravinski Hospital.
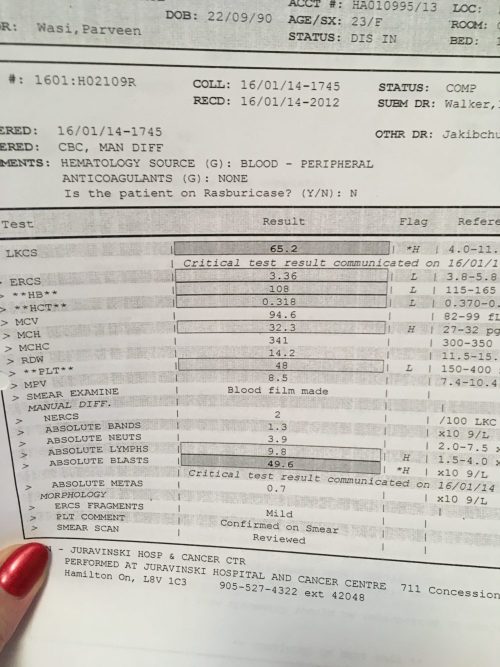
Upon arrival, she was acutely unwell and her WBC count had risen to 65. She was in DIC with an INR of 1.9, fibrinogen level of 1.4 which fell to 0.8 the following day, as well as an elevated PTT level. She remained oliguric and developed respiratory distress requiring more oxygen. She was transferred to the ICU for intensive monitoring.
Her course in hospital included:
Hematology- given her elevated creatinine, oliguric state and dialysis dependency, Miss Dickson received induction chemotherapy with daunorubicin dose reduced 50% as well as continuous infusion cytarabine. Ultimately, her cytogenetics returned which showed a translocation of 9,11 as well hypodiloidy in chromosomes 1,8,13,14,19,21 and 22 demonstrating complex cytogenetics. Her siblings were typed and unfortunately not suitable donors and therefore, a worldwide search has been initiated. Her day 14 marrow was empty. At this point another bone marrow aspirate and biopsy were done with marrow showing 10% blasts. The flow cytometry showed 6% blasts and the biopsy still pending. In discussing with Candace and her family , it was unclear whether this represented a recovering marrow or persistent Leukemia. The plan was to wait until the neutrophil count fully covered and move forward with another bone marrow aspirate and biopsy.
Infectious disease- Miss Dickson arrived to the Juravinski hospital having already started Tazacin. She developed a fever following her induction chemotherapy. This was culture negative. A source was not identified. She was changed to meropenem and defervced. This was stopped at count recovery and she was not stepped down to oral antibiotics.
Renal- Miss Dickson was believed to have acute kidney injury secondary to tumor lysis at presentation. In total, she received 3 dialysis treatments and then began spontaneously voiding. She was in a polyuric state for approximately 2 weeks following her dialysis but this has completely resolved and her creatinine level is in the mid 70s.
Thrombosis- Her initial CT scan of the abdomen revealed a thrombus in the portal vein. She then developed a right sided pleuritic pain during her induction treatment. Given her nephrology issues, there was some reluctance to move forward with a CT scan and had a VQ scan which was consistent with a PE. Once her platelets recovered she was initiated on full dose fragmin.
Breast mass- Miss Dickson developed a breast mass, hydronephrosis as well as a large abdominal mass which is likely related to the monocytic variant of her Leukemia. Her breast mass resolved following initiation of chemotherapy. She was discharged home when her neutrophil count recovered. She will follow up with Dr. Walker in the Cancer Center next week.
K.Kolm (NP)dictating for Dr. Kylie Lepic (MD)
03/03/14
